COVID-19 Outlook: Preparing for the Holidays
Editor’s Note: This blog post was updated on Nov. 12, 2020 at 5:00 p.m. to reflect our suggested quarantine timeline after the Thanksgiving holiday and clarify the data around COVID-19 infection rates in children as compared to adults.
Starting this week, we are changing the format of our blog posts. We’ll now start with a brief highlight of the key findings from our weekly COVID-Lab county-level forecasts, then move on to discuss emerging questions and challenges that are before us. So here goes.
Key data and COVID-Lab findings this week:
- Hospitalizations, ICU admissions and ventilator use are now increasing throughout all 50 states. In every Midwestern state, COVID-19 patients are occupying more than 25% of ICU beds.
- In four states—Montana, New Mexico, North Dakota and South Dakota—COVID-19 patients are occupying 50% or more of ICU beds. We suspect that in many localities across these states, ICUs are near, at or over capacity.
- We are forecasting substantial growth in case incidence over the next four weeks in the Northeast down through the Mid-Atlantic region, where dire trends previously seen in the Midwest have now set in. Mitigation efforts in and around New York City and Boston have slowed but not abated the growth in hospitalizations and ICU admissions in these cities.
- We are seeing some evidence that areas in Wisconsin, one of the earliest states to see explosive growth this fall, may be nearing a peak in case incidence, even as hospitalizations and ICU admissions have not yet stabilized.
- On the West Coast, we project that major cities in California will have significant case growth into mid-December, as will Portland and Seattle.
- At least half of the 819 counties for which we project case counts each week now have an instantaneous reproduction number greater than 1.25; a similar majority have testing positivity rates over 9%.
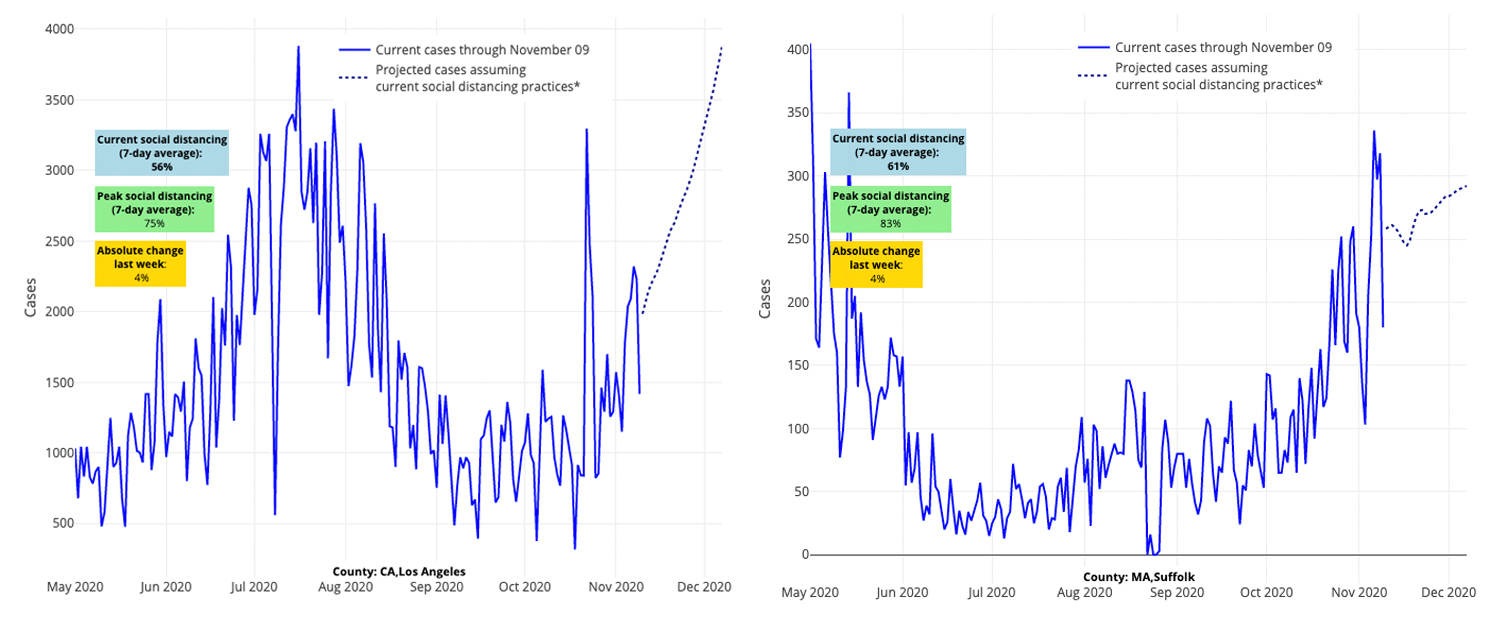
Above are the projections for Los Angeles County in California (left) and Suffolk County (Boston) in Massachusetts (right).
Last week, while we were distracted by the presidential election, COVID-19 transmission rates continued to accelerate across the country. The nearly universal rise in statewide hospitalization rates, particularly in our colder regions, is a pattern that will grow as we move into the holiday season.
It’s Time for Our Leaders to Act
We believe strongly the time is now for action by our policymakers. In the face of national emergency during which hospitals are being overrun across the country, we urgently need a public response from our leaders. There is no area in the country that is immune from this urgent call for sensible action to protect essential workers, teachers and school staff, health care systems and families.
Our framework for public policy action proposes immediate action beginning Nov. 16 and extending to after the holidays. The urgency of the Nov. 16 deadline reflects the window for a sufficient quarantine of most families in preparation for Thanksgiving. A quarantine period of at least one week after Thanksgiving would allow communities without accelerating transmission to assess and consider a potential short-term lightening of restrictions prior to the late-December holiday season. We also advise a similar pre-post quarantine period for Christmas time and New Year’s.
Our quarantine recommendations include requiring employers to move all non-essential employees to remote work. Gathering sizes would be limited. Bars and restaurants would be restricted, by occupancy or curfew or both. Civil penalties for those who actively defy public health guidelines would be enforced, particularly businesses operating in conflict with public health regulations, and for those (personal or commercial) actively flouting gathering size limitations. We are not focusing on family gatherings—we mean the large holiday parties and their venues.
What Accelerating Nationwide Transmission Rates Mean for Schools
More and more children, particularly older youth, are testing positive, and this increase can accelerate transmission to older adults who are more susceptible to severe infection—different transmission dynamics than we observed last spring.
We are now recommending that in areas with rapidly accelerating transmission rates (such as the Philadelphia region) schools, or families voluntarily, revert students to online learning beginning Nov. 16 until at least one week after Thanksgiving. This move to virtual learning should be prioritized for students in middle and high school. While we have seen increasing infection rates among child care and elementary-aged youth, their relative contribution to community burden of infection remains small. Therefore, decisions about distanced learning for younger children should be made at a local level and be responsive to the identification of linked transmission within school settings in that community.
There might be a brief period for students to return to the classroom in December between holidays, but in areas now beset with runaway transmission, they would likely opt to continue virtually until January. This a way to approach the upcoming holiday season that could balance the risk of introducing larger numbers of infected children/staff into school with the desire to maximize the time for in-person learning. It provides the opportunity for local officials to work with their local health departments to strategically use time-limited windows of virtual learning to respond to community transmission rates and lessen pressure on local health care systems.
Why this shift in guidance? Until now, protocols that reopened schools have been successful in preventing linked in-school transmission. Unfortunately, overall infection rates in children are rising in many areas of the country. At Children’s Hospital of Philadelphia, PCR test positivity rates this past weekend surpassed 15%, a number that nearly doubled in a week.
It is likely that many of these youth who are students were exposed to SARS-CoV-2 outside of school, at informal gatherings or other non-school-related activities. We assume that Halloween weekend events led to many breaches in social distancing, fostering rapid viral transmission between children, teens and adults. All along we have worried that increased pressure from rising community incidence would lead to linked in-school transmission. We have heard reports of linked transmission events over the last two weeks in southeastern Pennsylvania schools and New Jersey has reported 36 school outbreaks to date. It is likely that in the coming weeks, transmission in schools and around school-related activities will contribute to increasing community spread during the height of this crisis.
We know that many parents and students wish to continue in-school learning because they are appropriately concerned about the negative consequences of keeping youth out of school, such as inability to learn virtually and the psychological effects of isolation. These worries are valid, and we have had similar concerns throughout this pandemic.
Until now, we have aimed to guide schools on best practices for achieving in-person education as much as possible. But we currently find ourselves in a no-win situation. In some locations, hospitals have reached capacity for caring for patients, both with and without COVID-19. With colder weather our models predict that incidence rates will continue to rise, which means the demand for hospital beds will only grow. Certainly this week’s news of a vaccine on the horizon has instilled much optimism, but unfortunately it won’t arrive in time to shift the fundamental dynamics of the coming weeks. Therefore, we advise that in addition to businesses, schools and families now also must commit to short-term adjustments to activities to allow us to navigate this extremely high-risk period so that we can more quickly return to these activities thereafter.
Understandably, families are concerned that once their school makes the decision to return to virtual instruction, then rising hospitalization and infection rates would make it difficult to reopen in the near-term. While youth are clearly contributing to the spread of this virus, we do need to rally around the likelihood that while in-school transmission is happening, it’s far less than in other sectors of society. That knowledge could help us to return even more students to the classroom after the new year, and potentially many to full in-school instruction by the spring, once the strain on our hospitals is relieved. On the other side of this current time-sensitive crisis, we would advise that the sequence of mitigation measures in communities feature school closures as a last resort intervention, reserved only for emergency situations.
Our Guidance for the Holidays
On a personal level, the most prudent thing that families can do this holiday season is choose not to gather in person with their older higher-risk relatives. However, this pandemic has taken such an emotional toll, on children and seniors alike, that we suspect many families will likely take the risk of gathering. For those that do, outdoor events are safer than indoors, and conscientious spacing of older vulnerable individuals from the rest of the family will be important. But even more important is a commitment to quarantine before visiting family.
Moving Beyond This Crisis Point
Will these measures, if adopted synchronously, work to reduce community transmission? It will take time, as this wave has built a head of steam—much like it did in the spring—to subside. But should people agree to hunker down for a bit, it will alleviate the rapid pace of increasing COVID-19 hospitalizations, as well as potential flu infections, this holiday season.
This is a very sobering moment, as we are witnessing our own region enter a new phase of the pandemic this week. But we remain hopeful, armed with the knowledge as pediatricians, infectious disease experts, and public health professionals that school breaks during prior flu seasons beginning before Christmas have meaningfully interrupted transmission. And we believe that if families can hunker down for the next six weeks so we can ease the pressure currently being put on our hospitals, we can get to the other side of this crisis point.

